



Angiosarcoma
Introduction
The word sarcoma is Greek in origin and means "fleshy growth." Sarcomas are a group of soft tissue tumors that can occur in almost any portion of the body. Sarcomas encompass a broad range of tumors with over 70 subtypes. Each of these subtypes has individual features that make it unique. Jemal et al estimate there will be 9420 new sarcoma cases in 2005. This means that of the over 1.3 million cancers diagnosed in 2005, sarcomas will comprise about 0.7% of all these cancers (Jemal 2005). Classification of sarcomas is traditionally based on the tissue of origin, but is increasingly based on chromosomal abnormalities and other molecular markers.
Angiosarcomas are malignant sarcomas of vascular endothelial cell origin. Endothelial cells make up the lining of vessels. Angiosarcomas can occur in any region of the body, although they are most commonly located in the skin, breast, liver, and deep tissue. Cutaneous angiosarcomas, which are angiosarcomas of the skin, are commonly found in the face and scalp region (Holden 1987 and Morales 1981). Approximately 60% of all angiosarcomas are cutaneous. Soft tissue angiosarcomas account for up to 25% of these tumors, and breast angiosarcomas account for roughly 8% of angiosarcomas. Overall, angiosarcomas account for 1-2% of all sarcomas (Enzinger 2001 and Brennan 2001).
Angiosarcomas may present without an inciting cause (de novo), in chronically lymphedematous limbs (Stewert 1948), or in areas previously treated or exposed to radiation. These rare tumors have also been associated with some cancer causing materials such as vinyl chloride, arsenic, and thorium dioxide (Kojiro 1985, Creech 1974, Hozo 1997, Heath 1974, Falk 1979, and Nanus 1987).
How Does Angiosarcoma Present?

Angiosarcomas may present in a variety of manners. They may have an appearance suggesting infection, bruising, soft tissue mass, or a blood vessel like lesion (Greist 1978, Forman 1966, and Mahorner 1968).
Angiosarcomas are rarely associated with major vessels, and are uncommon in children. Several broad classifications have been identified to divide these tumors into categories based on the presenting clinical scenario (Enzinger 2001):
- Cutaneous angiosarcoma without associated lymphedema
- Cutaneous angiosarcoma with associated lymphedema
- Primary breast angiosarcomas
- Angiosarcomas of the deep soft tissue
- Radiation-induced angiosarcoma
- Angiosarcoma associated with foreign material
Importantly, however, the diagnostic methods, imaging techniques, treatment, and prognosis for these angiosarcoma subcategories are roughly equivalent.
Cutaneous Angiosarcoma Without Associated Lymphedema

Cutaneous angiosarcoma is the most common type of angiosarcoma. This accounts for roughly 60% of the angiosarcomas diagnosed each year (Morgan 2004). They most commonly affect older male patients and are typically located in the head and neck area (Holden 1987). Approximately 50% of the cutaneous angiosarcomas are located in the face and head and neck region (Weiss 2001). Cutaneous angiosarcoma may begin as ill-defined bruise like areas with raised borders, appear ulcerated, or nodular.
Microscopy
When assessed under a microscope angiosarcomas may appear like normal tissues (well to moderately differentiated), or vaguely resemble native tissues (poorly differentiated). Angiosarcomas may be classified as Grades I, II, or III. This correlates with well-differentiated, moderately differentiated, and poorly differentiated tumors respectively. These grading systems are used for many tumor types. However, regardless of tumor grade, angiosarcomas tend to be aggressive.
Angiosarcomas may form distinct blood vessel like (vascular) channels that are irregular in size and shape. Angiosarcomas may initially appear to be hemangiomas, a benign type of blood vessel tumor. However, a key difference is that the angiosarcoma vascular channels disrupt tissue planes, and form a connecting network of sinusoids or pools. Poorly differentiated angiosarcomas may require specific staining techniques to aid in identification.
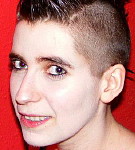
Cutaneous angiosarcomas may initially be perceived as benign or non-cancerous. This subtle development may lead to a delay in patients consulting a health care professional. Persistent or expanding bruises lasting longer than normal trauma related bruising suggests an underlying problem. This is particularly the case if there is bruising associated with a nodule (Figure 1). Pawlik et al reported that clinical signs existed an average of 5.1 months prior to diagnosis for scalp angiosarcomas, but in some, signs were present up to a year before diagnosis (Pawlik 2003). This tendency for delay is evident in most series investigating angiosarcomas.
Physical examination is not a reliable method to determine the overall extent of cutaneous lesions. Angiosarcomas are often multifocal which complicates therapeutic options. It may not be possible to determine if there is distant or even regional spread of disease by physical exam alone.
Cutaneous Angiosarcoma With Associated Lymphedema
In 1948 Stewart and Treves described six patients who developed vascular sarcomas following radical mastectomy and axillary lymph node dissection for breast carcinoma (Stewart 1948). The common factor in these patients was upper extremity lymphedema, or swelling of the arm. This occurred due to removal of the lymph nodes in the axilla or armpit. Angiosarcoma in the setting of lymphedema has since been called Stewart-Treves Syndrome. Over 300 cases of angiosarcoma related to chronic lymphedema have been reported (Roy 2004). Case reports following lymph node dissection for carcinoma of the penis, lymphedema of unknown cause (idiopathic), traumatic lymphedema, and lymphedema associated with parasites have also been described (Hallel-Halevy 1999, Sinclair SA 1998, and Komorowski 2003). The precise cause of angiosarcoma in the setting of lymphedema is still unknown.
Etiology of Stewart-Treves Syndrome
Theories on the cause of angiosarcomas in the face of lymphedema vary. Some authors propose that decreased clearance of the extremity lymph my expose the surrounding tissue to cancer causing agents. Others propose that removal of the lymph nodes creates a stimulant for growth of new vessels, which then leads to malignancy. Growth factors from surrounding tissues play an important role in the theory. Schreiber et al proposed that the lymphedematous state creates an "immunologically privileged site". This means that the area is remote and without access to the patient's ability to repair genetic mutations. Irradiation then could act as an additive genetic insult or simply perpetuate the lymphedematous state

Ninety percent of all angiosarcomas associated with lymphedema occur in women who have undergone mastectomy (Woodward 1972). The risk of Stewart-Treves syndrome is estimated to occur between 0.07% and 0.45% of women who undergo removal of the breast (Fitzpatrick 1969). In the few mastectomy patients in whom this occurs, angiosarcoma typically develops within 10 years of mastectomy. The appearance of this form of sarcoma, however, may be as early as four years or as late as 27 years after breast removal.
When angiosarcoma is associated with idiopathic or congenital lymphedema these tumors affect patients at a younger age, but take longer to develop overall. Most patients are in their fourth or fifth decade and have had significant lymphedema for over 18 years (Enzinger 2001).
These lesions typically appear as eccentric purple lesions superimposed on brawny non-pitting edema of the affected extremity. These lesions may progress to large palpable nodules with ulceration and weepy discharge. Patients with new bruising or nodules on an extremity with lymphedema should seek medical attention. Microscopically these lesions are similar to cutaneous angiosarcomas.
Angiosarcoma of the Breast

In general primary sarcomas of the breast are very rare (Adem 2004). Primary angiosarcoma of the breast, or angiosarcoma without other causes, accounts for up to .05% of all breast cancers. This amounts to one case of primary angiosarcoma of the breast per 2000 breast cancers diagnosed each year (Enzinger 2001). This tumor is often more aggressive than the more common types of breast cancer. Primary angiosarcoma of the breast will usually occur between the third and fourth decades of life in women only. These tumors may initially present with a deceptively bland appearance. However, they are typically rapid growing lesions that can cause diffuse enlargement of the breast (Johnson 2002). The breast may demonstrate blue-red discoloration of the skin, but these tumors are typically deep in the soft tissue. These cancers may encroach on the overlying skin, but almost never invade the chest wall muscle.
Angiosarcoma of Soft Tissue

Up to 25% of all angiosarcomas will be soft tissue tumors. These tumors may occur at any age and have a roughly equal distribution between men and women. About one third may be associated with other conditions such as inheritable genetic diseases (Meis-Kindbolm 1998). Neurofibromatosis, Klippel-Trenaunay Syndrome, Maffucci Syndrome, and other neoplasms are some conditions associated with soft tissue angiosarcomas. Soft tissue angiosarcomas are most commonly found in the extremities or the retroperitoneum.
These tumors will not typically present with the findings seen with cutaneous angiosarcomas. These tumors will typically present as a mass in the extremity, or by symptoms caused from compression or invasion of structures within the abdomen. Abdominal angiosarcomas may grow to a large size before causing symptoms. Large size may be associated with other clinical findings including destruction of platelets, heart failure, or spontaneous bleeding, particularly in the young.
These lesions commonly have an epithelioid appearance on histology, and up to one-third may express cytokeratin, a protein common to non-sarcoma cancers. These findings can make it difficult to distinguish angiosarcomas from other cancers. Diagnosis of soft tissue angiosarcomas may not be possible until other histochemical stains are able to differentiate the angiosarcomas from other types of tumors.
Angiosarcomas of specific organs including liver, spleen, and heart have been described. These organ-specific angiosarcomas may be considered as a sub-group of soft tissue angiosarcomas. Their treatment may be individualized, but overall principles are still germane.
Radiation-Induced Angiosarcoma

In the past, radiation induced angiosarcomas have commonly presented as intra-abdominal or abdominal wall masses following radiation treatment for gynecologic malignancies. A small number of cases have been reported after irradiation for other conditions, including benign processes (Westerberg 1989). However, in the last several years more than 100 angiosarcomas involving the skin or breast parenchyma have been reported in women undergoing breast-sparing surgery and irradiation (Monroe 2003). Marchal et al reported nine cases in 18,000 women treated with breast conserving therapy and external beam irradiation. This accounts for roughly .05% of patients undergoing a breast-conserving strategy for breast cancer.
These lesions are characterized by ecchymoses or thickening of the skin with elevated lesions in a radiated area.
The lesions are typically painless and often multifocal. Angiosarcomas may present as a single bruise like area or with diffuse swelling of the entire breast. Patients may initially mistake these findings to trauma contributing to delay in seeking medical attention.
Recent reports of radiation induced breast angiosarcoma observed on average an interval of 4-7 years prior to development (Billings 2004, Brenn 2005, Feigenberg 2002, and Pierece 1992). This interval may be longer and range greater than ten years.
Angiosarcomas related to lymphedema, in contrast, have longer intervals before development. On average, this interval is more than ten years (Laskin 1988, Davidson 1986). This interval, whether associated with lymphedema or radiation induced angiosarcoma does not appear to affect prognosis.
Angiosarcoma Associated with Foreign Material
Angiosarcomas may rarely develop in response to, or develop associated with, foreign material. Approximately 20 cases of angiosarcoma caused by foreign body have been documented (Joo 2005, Ben-Izhak 1992, and Jennings TA 1988). This form of angiosarcoma may be seen in patients with dialysis shunts made of Dacron. There have also been reports of angiosarcomas developing in response to surgical material left in abdomens of patients previously operated on. Overall these Angiosarcomas behave similarly to soft tissue angiosarcomas. The foreign material should be removed along with the tumors in these patients if possible.
Imaging of Angiosarcoma

Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) are the imaging modalities of choice to evaluate and follow angiosarcomas or to look for distant spread of disease. CT findings of angiosarcomas typically reveal a nonspecific soft tissue mass with attenuation comparable to muscle (Sugita 2002). MRI offers the advantages of more defined tissue planes and no exposure to radiation. MRI is the method of choice to evaluate the tumor response to preoperative radiation or chemotherapy. Reported angiosarcoma findings on MRI may be of a nonspecific mass with signal intensity similar to that of muscle on T1-weighted images and very high signal intensity on T2-weighted images. Hypointensity on both images may suggest organized hemorrhagic focus. MRI is capable of detecting the vascular channels and spaces that suggest the diagnosis of a vascular lesion (Coldwell 1989). In a study of eight patients with angiosarcoma of the scalp, Isoda et al found that in four patients, the tumors were larger on MRI than clinical inspection (Isoda 2005). Other consistent findings in this study were T2-weighted enhancement with fat saturation and contrast-enhanced T1-weighted MRI imaging with fat saturation demonstrating tumors invading into the subcutaneous fat and muscle clearly. MRI may be helpful in pre-surgical planning.
Mammograms performed for angiosarcoma of the breast may reveal skin thickening or superficial mass, but up to 33% of patients with this form of angiosarcoma will have no findings on this imaging method (Liberman 1992). These lesions may be markedly enhance on T2 weighted MRI images (Marchant 1997). This means MRI may be useful for breast angiosarcoma. Positron Emission Tomography (PET) scans measure metabolic activity of tumors and may become an additional imaging technique to correlate with tumor grade. There is evidence that PET imaging is useful in some types of sarcoma, however, there are no large studies to date that report the uniform use of this new form of imaging modality in angiosarcomas (Goldstein 2005 and Hicks 2005). Freudenberg et al have reported a case of cardiac angiosarcoma diagnosis through PET scan when both MRI and CT were unable to differentiate a benign versus a malignant lesion (Freudenberg 2002).
Angiosarcoma Genetics and Inheritance
Many sarcomas are known to have chromosomal or genetic abnormalities. To date there are no specific identifiable chromosomal abnormalities associated with angiosarcoma, but with new technology available investigations into these matters are ongoing. There are also rare instances of angiosarcomas developing in family members without direct evidence of any environmental exposure.
Genetic and Chromosomal Characteristics
Angiosarcoma has been associated with both chromosomal abnormalities and inheritable genetic diseases. Frequent chromosome abnormalities are gains in the normal number of two of each chromosomes 5, 20, and 8 and losses of chromosomes 7, 22, and the male Y chromosome. Baumhoer et al evaluated four angiosarcomas of the breast. Though there were several chromosomal abnormalities, gains in chromosome 8 were the most common. Genetic diseases associated with angiosarcomas include Klippel Trenaunay Syndrome, Von Hippel Landau disease, and Von Recklinghausen’s neurofibromatosis (Lederman 1987, Martz 1992, and Meis-Kindblum 1998). There have also been a few isolated reports of angiosarcomas among primary relatives without obvious cause (McIntosh 2005 and Khan 2004). This suggests a rare inheritable variant of angiosarcoma or possible unknown exposure to an angiosarcoma-causing agent among family members.

Histology of Angiosarcoma
All of the angiosarcoma "types" have similar findings when looked at under a microscope. Pinocytotic vesicles and Weibel-Palade bodies (tubular structures commonly found in normal endothelium) may be identified pathologically. These tumors demonstrate vascular spaces lined by abnormal tumor cells. Tumors are often characterized as either low-grade or high-grade tumors.
Low-grade or well-differentiated (less malignant looking) lesions have vascular spaces lined by large plump cells that project into surrounding tissue.
High-grade or poorly differentiated lesions tend to be less vessel-like and more cellular. Hemorrhage into the surrounding tissue is coined "blood lakes" and often seen in high-grade angiosarcoma. The cells in high-grade tumors don’t resemble normal vascular tissue or cells.
Trends in Immunohistochemical Markers
Factor VIII-associated antigen and CD34 represent the most common immunohistochemical markers associated with angiosarcoma. CD31, a platelet-endothelial cell adhesion molecule, may be used, and is a more accurate antigen for endothelial differentiation (DeYoung 1995). Although many papers comment on the grade or histological subtype of angiosarcomas, these factors are typically equivocal prognostic indicators (Miettinen 1994). In the majority of cases the tumor grade is high. Other features play a more dominant role in outcome. Occasionally pathologists will comment on patterns of growth. These patterns are referred to as angiomatous pattern with epithelioid features, a spindle cell pattern, or an undifferentiated or solid pattern. It is not uncommon to find different patterns mixed within the same tumor.
Angiosarcoma Treatment
Angiosarcomas ideally require medical attention from a knowledgeable experienced multidisciplinary medical center team. This team includes surgeons, medical and radiation oncologists. Decisions on whether to proceed with surgery initially, or by other modalities alone or with surgery is made by this team and the patient.
Surgery
Surgical excision is the mainstay of curative treatment for all forms of angiosarcoma. Even if there is distant spread, surgery may be offered to control the primary cancer site. Angiosarcoma can be difficult to assess by physical examination alone. The area excised may be larger than initially suspected. This is particularly true when dealing with angiosarcomas of the scalp. Preoperative mapping may provide a better surgical result (Bullen 1998). This means biopsies are taken around the tumor to assure the best chance of complete removal. This may be done in the office before completely removing the cancer or in the operating room at the time of intended resection.
Surgical Options for Scalp Angiosarcoma
Pawlik et al reviewed their experience with scalp angiosarcomas (Pawlik 2003). They reported an elderly male predominance consistent with other reports. They also found that surgical margins were frequently positive and frozen section had a poor sensitivity when compared to permanent analysis. To this end, they recommend delayed reconstruction as a surgical option. Using skin substitutes until final margins are clear or surgical possibilities are exhausted was a viable surgical approach. This review found that low T stage, younger age, and whole field external beam radiation correlated with improved survival.
Options available when considering surgery for angiosarcomas of the breast are mastectomy versus local resection. Mastectomy without lymph node dissection is the operation that is selected usually. These tumors do not typically involve the regional lymph nodes reducing the need for axillary lymph node dissection. Long-term survival of patients with angiosarcoma developing in the setting of lymphedema have typically been treated by radical surgery. This may include amputation of an involved extremity. Less aggressive surgery and radiation as a sole therapy are associated with higher recurrence rates (Woodward 1972 and Sordillo 1981). This may be due to the often more extensive local state of disease than initially perceived leading to residual disease after resection or radiation. For all angiosarcomas the primary surgical goal is to remove the entire cancer with a rim of normal tissue if possible.
Neo-Adjuvant and Adjuvant Therapy
Neo-adjuvant therapy refers to giving chemotherapy, radiation, or both prior to attempting surgical resection of a tumor. Adjuvant therapy means these treatments are given after surgery when surgery has removed all signs of visible tumor. Doses of radiation and chemotherapy given in the neo-adjuvant setting are typically less than those given after surgery. Radiation is used in local tumor bearing regions, whereas chemotherapy is used to treat systemic spread of disease. Most specialists reserve preoperative chemotherapy for patients with lesions that are unresectable or in situations where chemotherapy along with radiation may help shrink a large or unresectable tumor. Reduction of tumor size in a preoperative setting may allow for a more cosmetically pleasing result in areas where this is important.
The chemotherapy agent of choice has traditionally been doxorubicin (Fury 2005). Some centers treat with multiple chemotherapy agents, a method that may reduce the overall amount of each drug dose given and thus decrease each agent’s associated individual toxicity. Traditionally, the combined chemotherapy agents for sarcomas in general have been mesna, doxorubicin, and ifosfamide (MAI). If no response is seen, other agents may be tried. Recent studies have evaluated paclitaxel as a single agent (Fata 1999). This drug may have substantial activity against angiosarcoma of the scalp or face, even in patients previously treated with chemotherapy or radiation therapy. If good response is seen with pre-operative treatment, the same drugs may be used after surgery.
Paclitaxel Based Chemotherapy
Some studies have shown a significant increase in disease free survival in patients treated with head and neck, or scalp angiosarcomas. Fury et al reported increased disease free survival in angiosarcomas of the scalp compared to patients who were diagnosed with angiosarcoma below the clavicle (Fury 2005). This significant difference was not observed for non-paclitaxel regimens. Fata et al have also reported that paclitaxel has been reported to have activity against scalp angiosarcomas (Fata 1000). This group demonstrated an overall response rate of 89%, with a median duration of response of five months. Skubitz et al demonstrated major response to paclitaxel in five of eight patients with angiosarcoma (Skubitz 2005). Interestingly, only one of these patients had angiosarcoma of the scalp, while the others included soft tissue tumors and primary organ angiosarcomas. Many centers are now using paclitaxel as a first line agent in the treatment of angiosarcoma.
Angiosarcomas have been found to be sensitive to radiation. The use of irradiation in conjunction with surgery may result in a more functional and cosmetic outcome, however cosmesis should not be the primary concern. Pawlik et al found that external beam irradiation given to patients after resection correlated with improved outcome (Pawlik 2003). Irradiation to the remaining area may be offered when the primary tumor is unable to be completely resected. Pre-operative radiation may optimize surgical field and decrease radiation damage to healthy tissue (Monroe 2003). This treatment however may require plastic surgery assisted closure secondary to large defect. This therapy may cause a delay in planned surgery but there is no evidence this delay worsens outcome.
Surveillance
Patients with angiosarcoma should be followed closely in the post-operative period. As a rough guideline, once the patient has recovered from surgery, quarterly visits to the physician with or without imaging are typically warranted for the first two years. After two years, semi-annual visits are performed until the five-year anniversary. After five years annual follow up is performed. These time intervals will vary depending on each patient’s clinical situation.
Angiosarcoma Prognosis
It is not uncommon for patients with angiosarcoma to have distant spread at the time of diagnosis. Up to 50% of angiosarcoma patients may have distant spread of disease at the time of diagnosis. Metastases or spread away from the original tumor site are most commonly seen regionally in the lymph nodes, distantly in the lung, liver, or spleen, and sometimes in both regions. Even when these tumors are grossly and microscopically removed recurrence may occur at a later time. In this situation, most recurrences will usually develop within two years. Risk factors for recurrence or distal spread include delayed presentation, incomplete resection, and extensive primary disease.
Studies have shown that improved prognosis correlates with smaller tumors, the use of wide-field radiation therapy, and resection margins free of tumor (Fury 2005, Pawlik 2003, and Donnell 1981). Some studies show that slower dividing tumors, tumors with a low mitotic rate, may have a better prognosis (Morgan 2003 and Naka 1996). Mark and Maddox both reported better prognosis for lesions less than 5 cm (Mark 1996), whereas Holden et all found improved survival for tumors less than 10 cm (Holden 1987). The overall principle is that smaller tumors tend to have a better prognosis. This emphasizes the importance of early diagnosis.
Soft tissue angiosarcomas of the abdomen tend to have a worse prognosis. This is predominantly due to a location that may be difficult to examine and that presents later than other types of angiosarcoma. Situations where total removal of organ specific angiosarcoma (e.g. angiosarcoma of the heart) may lead to increased chance for recurrence.
Early diagnosis and treatment are the keys to cure for angiosarcomas. Recognizing the clinical signs and symptoms are important. Patients with long standing lymphedema or a history of radiation treatment should be vigilant and examined by a health care professional on a regular basis.
For most angiosarcomas, the tumor grade does not significantly affect prognosis. This may be related to the inherent behavior of angiosarcoma, regardless of grade. Overall, angiosarcoma tends to have a relatively poor prognosis. However, this is not necessarily true for angiosarcomas of the breast. For breast angiosarcomas, low-grade lesions have a better prognosis than high-grade lesions. The most common location for distal metastasis from breast angiosarcoma is the contra lateral breast (Monroe 2003).
Science & Research
The Liddy Shriver Sarcoma Initiative is funding a 2012 study on ROCK Inhibition as an Anti-Angiosarcoma Therapeutic.
Several laboratories are investigating the etiology (cause) of angiosarcomas. Laboratories have the advantage that predictable animal models of angiosarcomas exist. Because angiosarcoma is such a rare tumor, cure must be sought through clinical trials and from scientists in the laboratory.
Laboratory Science
Morgan et al injected the viral counterpart of a cellular proto-oncogene c-src into chick embryos (Morgan 2004). Injection of v-sarc resulted in the death of most embryos, but also large hemangiosarcomas over the injection site in many. This implicates a genetic role in etiology of malignant vascular tumors. One laboratory has found an association between cadherin expression and angiosarcomas. Cadherin is a cellular adhesion molecule that inversely correlates with tumor malignancy. Interestingly, endothelial specific cadherins (VE-cadherin) is low or absent in angiosarcomas. This protein may play an inhibitory role in tumor progression. Loss of these molecules may account for altered fibrinolytic activity and predispose to bleeding (Zanetta 2005).
Rathmell et al noted that the tumor of a patient with a retroperitoneal angiosarcoma demonstrated widespread up-regulation of the hypoxic response pathway as a mechanism of enhanced VEGF expression (Rathmell 2004). They hypothesize that disordered regulation of this pathway may result in angiogenic inducing factors such as VEGF and erythropoietin. This up-regulation may result in tumor growth. Both endothelial cells and red blood cells are exposed to high amounts of oxidative stress. Oxygen produces toxic free radical that may lead to damage of vessels and red blood cells. Lee et al found that malignant vascular tumors failed to express peroxidase II (PrxII) an enzyme that destroys reactive oxygen species, whereas benign vascular tumors did (Lee 2003). It is possible that the lack of PrxII in angiosarcomas may indicate oxidative damage as a contributing cause. Riddelliine is a plant derivative that is used as an herbal remedy in the southwestern USA. Studies have found that this agent alters hepatocellular and endothelial cell kinetics and may cause dysregulation of VEGF synthesis. This injury activated endothelium KDR/flk-1 leading to induction of sustained endothelial cell proliferation culminating in the development of hepatic angiosarcoma.
Future Horizons
Liposomal encapsulation is a method of incorporating the drug into a fat delivery system that acts as a slow releasing system that is less toxic to surrounding vessels and tissues. Liposomal encapsulation of doxorubicin may reduce cardiac effects seen in the standard form of the drug. Doxorubicin (a.k.a. adriamycin) has toxic effects on the heart muscle at cumulative doses of 450 mg/m2.
Paclitaxel, a chemotherapy agent commonly used in breast and ovarian cancer has substantial activity against angiosarcoma of the scalp or face (Choy 2001). This drug is a known antiangiogenic and may prove to be a beneficial chemotherapy agent in other areas of the body. Belotti et al have demonstrated this drug's effectiveness as an antiangiogenic (Belotti 1996). Antiangiogenic drugs cut off the blood supply to tumors. Investigations into the effects of antiangiogenic drugs are ongoing. It is possible that these drugs could have an effect on malignant vascular tumors. Currently trials employing antiangiogenic strategies against angiosarcoma are ongoing.
Thalidomide has been associated with tumor necrosis in small intestine angiosarcoma (Fraiman 2003). This drug was given under an experimental protocol and has also been approved to treat lesions associated with leprosy and multiple myeloma. It is notable that when taken during pregnancy as an anti-nausea medication severe birth defects were common. This agent has also been noted to be a potent antiangiogenic.
Conclusion
Angiosarcomas are a rare form of sarcoma that may occur in almost any location of the body. These tumors are aggressive and are ideally treated at an experienced cancer center, with a multidisciplinary approach. Better prognosis is associated with smaller size and free margins at the time of first surgery. New treatment options may include antiangiogenic, immunotherapy, and multi-modality treatment. Table 1 provides a list of questions a person may ask his or her physician concerning a diagnosis with angiosarcoma.
| Question | Response |
|---|---|
| What type of angiosarcoma do I have? | |
| How will I know if the cancer has spread? | |
| Will I need surgery? | |
| If surgery is required will a skin graft be necessary? | |
| What if there is residual cancer after my surgery? What should I watch for? | |
| Could radiation therapy be helpful? | |
| Could pre-operative chemotherapy or radiation be helpful? | |
| If my angiosarcoma is completely resected what should I watch for after surgery? | |
| How often will I need to see a physician after my surgery? |
Acknowledgements
H. Lee Moffitt Cancer Center & Research Institute: Division of Sarcoma and Soft Tissue Tumors, Division of Pathology, Division of Plastic & Reconstructive Surgery and Division of Breast Oncology & Surgery.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}